
- |
- |
- |
- |
- |
- |

Products
Clinical materials and methods
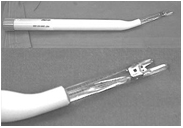 All operations were performed using the KnifeLight instrument, which is specially designed with a blunt tip and an inner U-shaped sharp cutting blade (Fig. 1B). The transverse carpal ligament was placed between the small blunt tips and cut between the inner sharp cutting blade. Between July 2003 and April 2005, 44 consecutive patients (50 hands) with clinically symptomatic and electrophysiologically confirmed CTS were enrolled in our study and underwent this procedure
All operations were performed using the KnifeLight instrument, which is specially designed with a blunt tip and an inner U-shaped sharp cutting blade (Fig. 1B). The transverse carpal ligament was placed between the small blunt tips and cut between the inner sharp cutting blade. Between July 2003 and April 2005, 44 consecutive patients (50 hands) with clinically symptomatic and electrophysiologically confirmed CTS were enrolled in our study and underwent this procedureAssessment method and follow-up action
Patients were asked to complete pre- and postoperative functional evaluations. The Michigan Hand Outcomes Questionaires (MHQ) was used to determine overall hand function, activities of daily living, work performance, pain, aesthetics, and satisfaction with hand function.
Surgical technique
 All operations were performed under sterile conditions using local anesthetic field block with 2% lidocaine with adrenaline. Asmall transverse line was drawn at the proximal wrist crease over the transverse carpal ligament, midpoint between the scaphoid and hamate bones. A second line was drawn along the radial border of the ring finger to intersect with the midpoint of the transverse line demarcated at the distal wrist crease (Fig. 2). A small transverse skin incision of approximately 10 mm in length was made to the ulnar side of this intersected point at the proximal wrist crease. This helps to avoid injury to the palmar cutaneous branch and the motor thenar branch of the median nerve.
All operations were performed under sterile conditions using local anesthetic field block with 2% lidocaine with adrenaline. Asmall transverse line was drawn at the proximal wrist crease over the transverse carpal ligament, midpoint between the scaphoid and hamate bones. A second line was drawn along the radial border of the ring finger to intersect with the midpoint of the transverse line demarcated at the distal wrist crease (Fig. 2). A small transverse skin incision of approximately 10 mm in length was made to the ulnar side of this intersected point at the proximal wrist crease. This helps to avoid injury to the palmar cutaneous branch and the motor thenar branch of the median nerve.